
Complement-Based Strategy Against CRC
- Martin Döhring

- 26. Sept. 2025
- 2 Min. Lesezeit
molecular-level therapeutic strategy to turn the complement system (C’) against colorectal cancer (CRC) cells so that the membrane attack complex (MAC, C5b–C9) lyses tumor cells. Here’s how that work:
🔬 Complement-Based Strategy Against CRC
1. The Problem
CRC cells often evade complement attack by:
Overexpressing complement regulatory proteins (CRPs) such as CD46, CD55 (DAF), CD59 (Protectin).
CD55 prevents C3/C5 convertase formation.
CD59 blocks MAC insertion.
Tumor microenvironment (TME) suppresses immune activation (Tregs, MDSCs, TGF-β, etc.).
Thus, complement is kept “off” on CRC cells, even when antibodies bind.
2. Therapeutic Strategy: Force MAC Formation
(a) Target CRC cells with antibodies that fix complement
Use monoclonal antibodies (mAbs) against CRC tumor antigens (e.g. CEA, EpCAM, HER2, EGFR, PD-L1) designed for strong C1q binding.
These activate the classical pathway → C3 convertase → C5 convertase → MAC.
(b) Block complement regulators on tumor cells
Inhibit CD55/CD59 using:
Blocking antibodies
siRNA / ASOs against CD55/CD59
CRISPR-based knockdown in experimental models
Without these, tumor cells lose their complement shield → MAC can assemble.
(c) Enhance complement amplification
Deliver recombinant C3/C5 convertase stabilizers (e.g. properdin analogs).
Use C5a receptor agonists to boost local complement activation (but balance against inflammation).
(d) Combination with Immunotherapy
Checkpoint inhibitors (anti-PD-1/PD-L1, anti-CTLA-4) unleash T cells → generate more antibodies → feed into complement activation.
Oncolytic viruses engineered to express complement-activating Fc fragments could also seed tumor lesions with complement triggers.
3. Molecular Cascade
Step 1: Antibody binds CRC antigen (CEA, EpCAM, etc.)
Step 2: C1q recruited → Classical complement pathway → C3/C5 convertases
Step 3: Block CD55/CD59 → convertases remain active
Step 4: C5 → C5b, recruits C6–C9 → MAC pores form
Step 5: CRC cell lysis (osmotic shock)
4. Safety Considerations
Risk: Excess complement = bystander damage to normal colon tissue.
Solution:
Tumor-targeted antibody delivery (bispecific mAbs, nanocarriers).
Local complement boosting (intra-tumoral injection of C5 agonists).
Check dosing carefully to avoid systemic complement storm.
✅ Summary:To overcome CRC tumors via complement:
Use complement-fixing antibodies against tumor antigens.
Inhibit CD55/CD59 on CRC cells.
Boost complement amplification locally.
Combine with checkpoint blockade or oncolytic virotherapy for synergy.


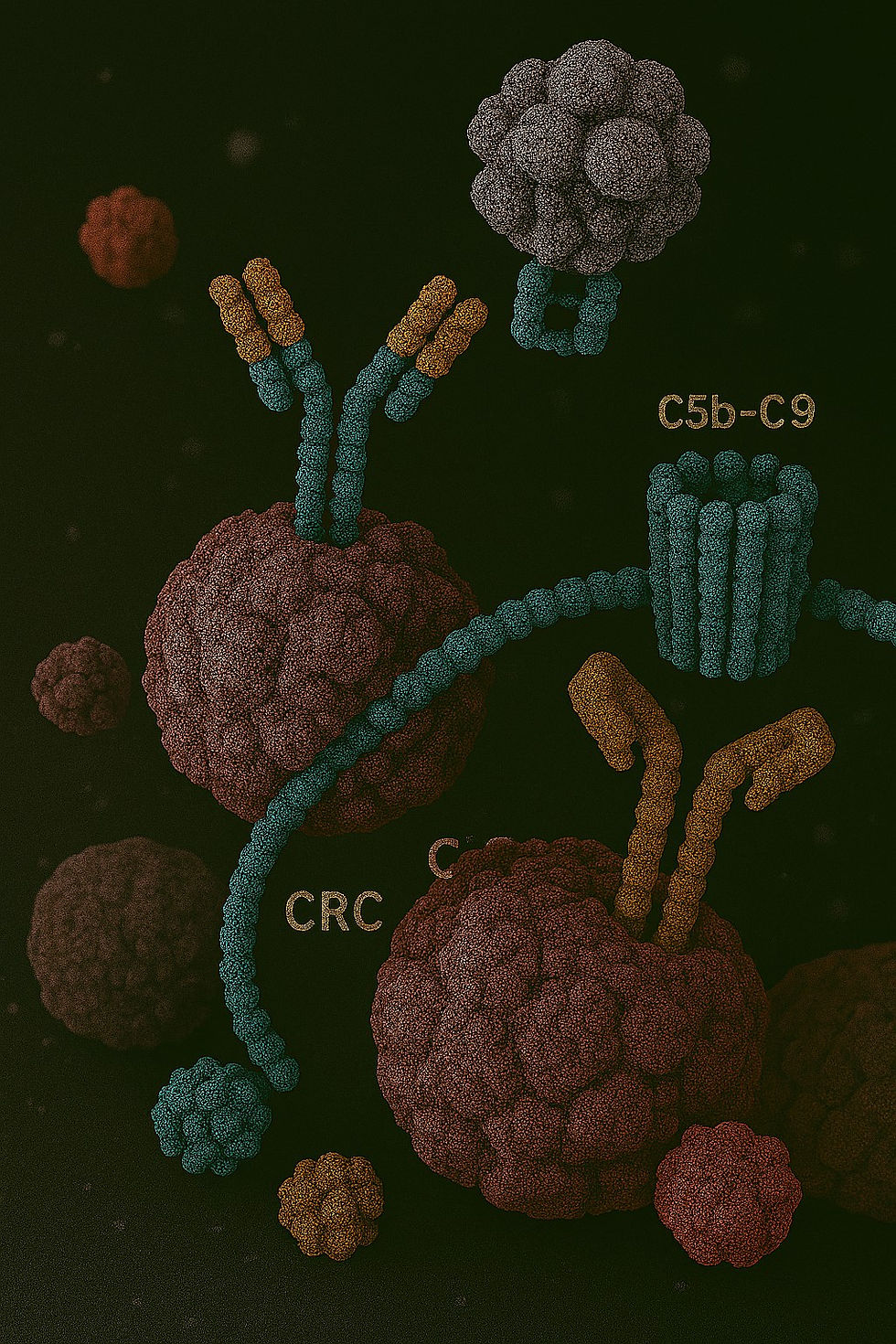
🧬 FOTOREALISTISCHE MOLEKULAR-VISUALISIERUNG
„Turning Complement Against CRC“ – MAC‑vermittelte Tumorzell-Lyse
🎨 Bildbeschreibung
...below is a compact, practical conceptual list of biomarkers and assay panels you can use to monitor complement activation, MAC formation, pharmacodynamics, and tissue/organ damage during preclinical or clinical development. I group markers by purpose, state the typical assay types, and give short rationales and sampling/interpretation notes.
Systemic complement activity (circulating)
Purpose: detect whole-body complement activation, consumption, and anaphylatoxins.
C3, C4 (total levels) — measure complement consumption.Assays: immunoturbidimetry/ELISA.
C3a, C4a, C5a (anaphylatoxins) — acute activation signals, correlate with inflammation.Assays: ELISA or multiplex immunoassay.
sC5b-9 (soluble terminal complex) — indicator of terminal pathway activation and ongoing MAC assembly.Assays: ELISA.
Bb / Ba (alternative pathway split products) — detect AP activation.Assays: ELISA.
Properdin — AP stabilizer; changes may indicate amplification.Assays: ELISA.
Functional hemolytic assays (CH50 — classical pathway; AH50/AP50 — alternative pathway)…